Dr. Anam Tariq continues the discussion about hypertension. In this session, Dr. Tariq discusses with Dr. Mobeen the management aspects of hypertension. Questions from the community members are used to address common clinical scenarios and potential approach to consider.
The topics discussed are related to the following questions:
Questions from René Gardner: With the new guidelines recommending <130/80. How aggressively are they with pursuing this? Especially in older patients.
Related questions:
Kathy RN AHA vs. JNC8 guidelines?
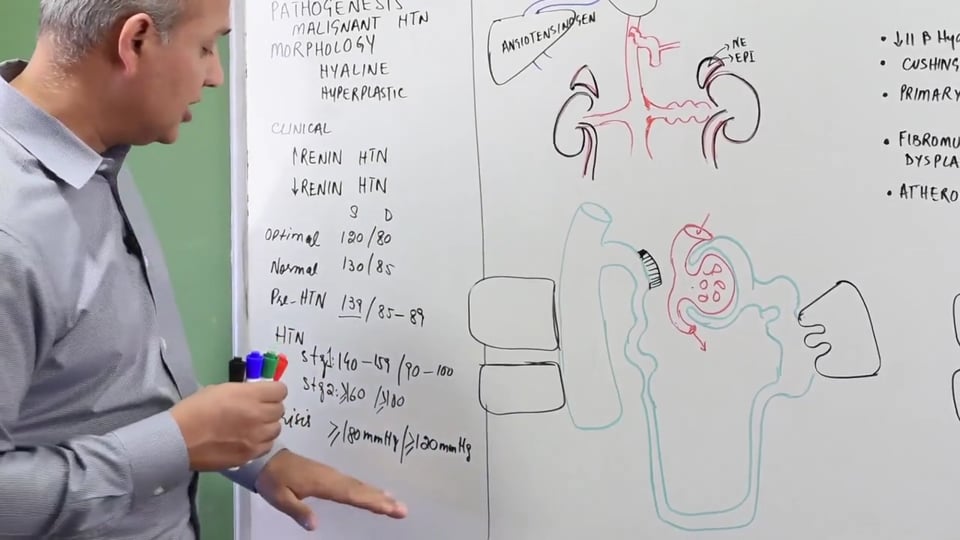
AHA: elevated BP >130/80, stage 1 >130/80
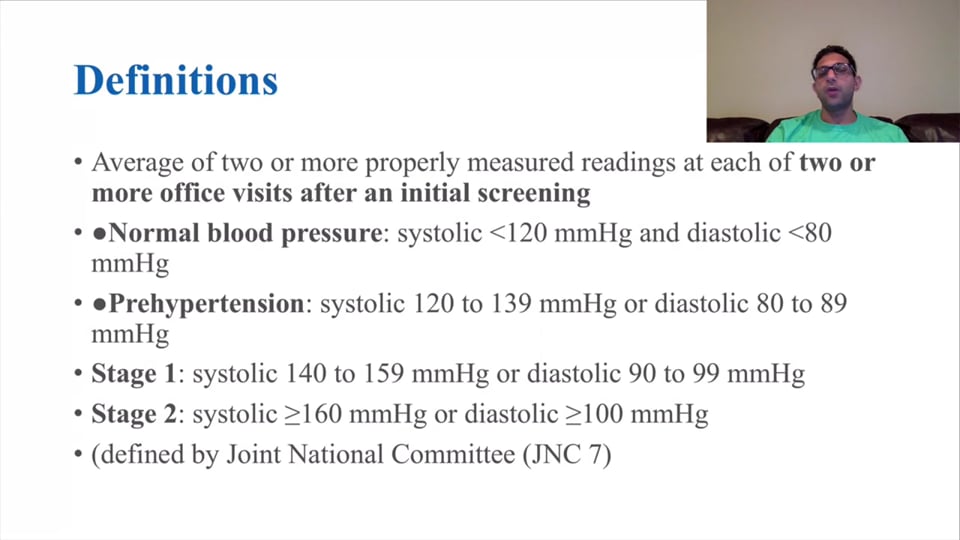
Dr. Tariq discusses the definition and stages of abnormal blood pressure, according to the American Heart Association (AHA).
Question from Kat Tugado: Good evening, I would like to hear her insights on the latest management in pediatric hypertension. Thank you.
Question from Bishal Baishya I have a question with 2 parts -
"When new JNC and AHA guidelines were modified to remove Prehypertension, and reduce the upper roof of normal limits.
1. How do clinicians and patient themselves target for a level of healthy BP and management of hypertension? Because new levels are more of just numbers a patient can just dream to reach. It does have a negative psychological impact that they shall be always be unfit.
2.Does it necessarily mean that they should touch this new lower levels to stay fit when by region and altitude they were acclimatise to 110 to 120 systolic and likewise near diastolic levels?"
Question from Robert Adams: Is there a common mistake you see more “rookie” practitioners make treating hypertension, and if so , how can we avoid it?
Question from DrAlkesh Patel: How u predict or judge intermediate htn or border line htn
And mostly what the causative agent what true managment
Marwan Hassan A Is it advisable to restrict table salt for HTN patients who are on a treatment plan?
Dr. Anam discusses the correct process of taking a person's blood pressure. We believe this is a process that is overlooked in the majority of clinical practice. We hope our audience will take special note of this process and make it routine for their clinical practice.
Dr. Tariq discusses the potential for precise medical practice by using ambulatory monitoring devices for hypertension.
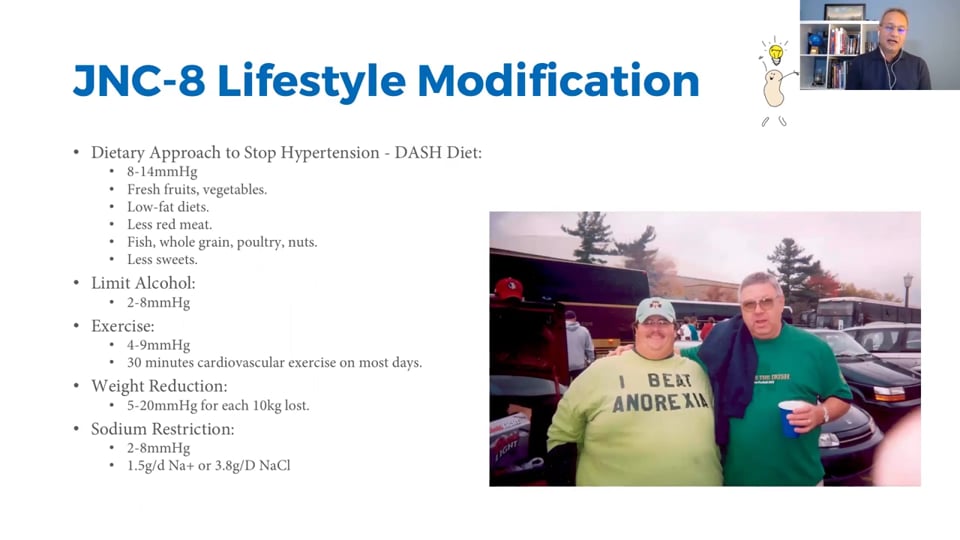
Question from Robert Adams: Is there good data for non pharmacological treatments like diet, exercise and increased higher quality sleep ? And what sort of reduction benefit might we expect from lifestyle changes , and over what time frame?
Questions from Robert Adams: A patient comes to you with a bp of 225/110 , how long would be an acceptable amount of time to get control of their bp and what might a reasonable bp be for them ?
Questions from Khaty RN: Patient with BP of 225/110 needs close monitoring and observation to prevent microvascular damage. PCP or family cannot manage unstable patients in the outpatient. That is why we refer to ED or cardiology.
Questions from Lee Ann Summers: does this person need to be sent to ED or can I start management in the outpatient setting?
Questions from Marlene Torres: Is it in the best interest of the patient to get a medication that will lower the blood pressure fast but possible give them rebound HTN? Or should be just give the patient HTN medication based on their ethnicity and bring them back in 1 week, so on and so forth so their BP comes down slowly instead of giving a quick result. I ask because this has been a blazing dispute between some providers in my clinic face.
Questions from Robert Adams: if this is chronic then they are no less stable than when they walked into your clinic to though, and probably much less stable if you begin aggressively lowering their bp secondary to hypo perfusing their brain and kidneys , the sepsispam trial might be able to offer us guidance on this in the inpatient setting
https://www.wikijournalclub.org/wiki/SEPSISPAM
Questions from Abdi Razak Yousuf Kahin: Why beta blockers are not a first line drug for HTN ?
Questions from Mohammad Salman: Resistant hypertension etiology and treatment plan.
Hypertensive urgency , emergency plus malignant Hypertension management.
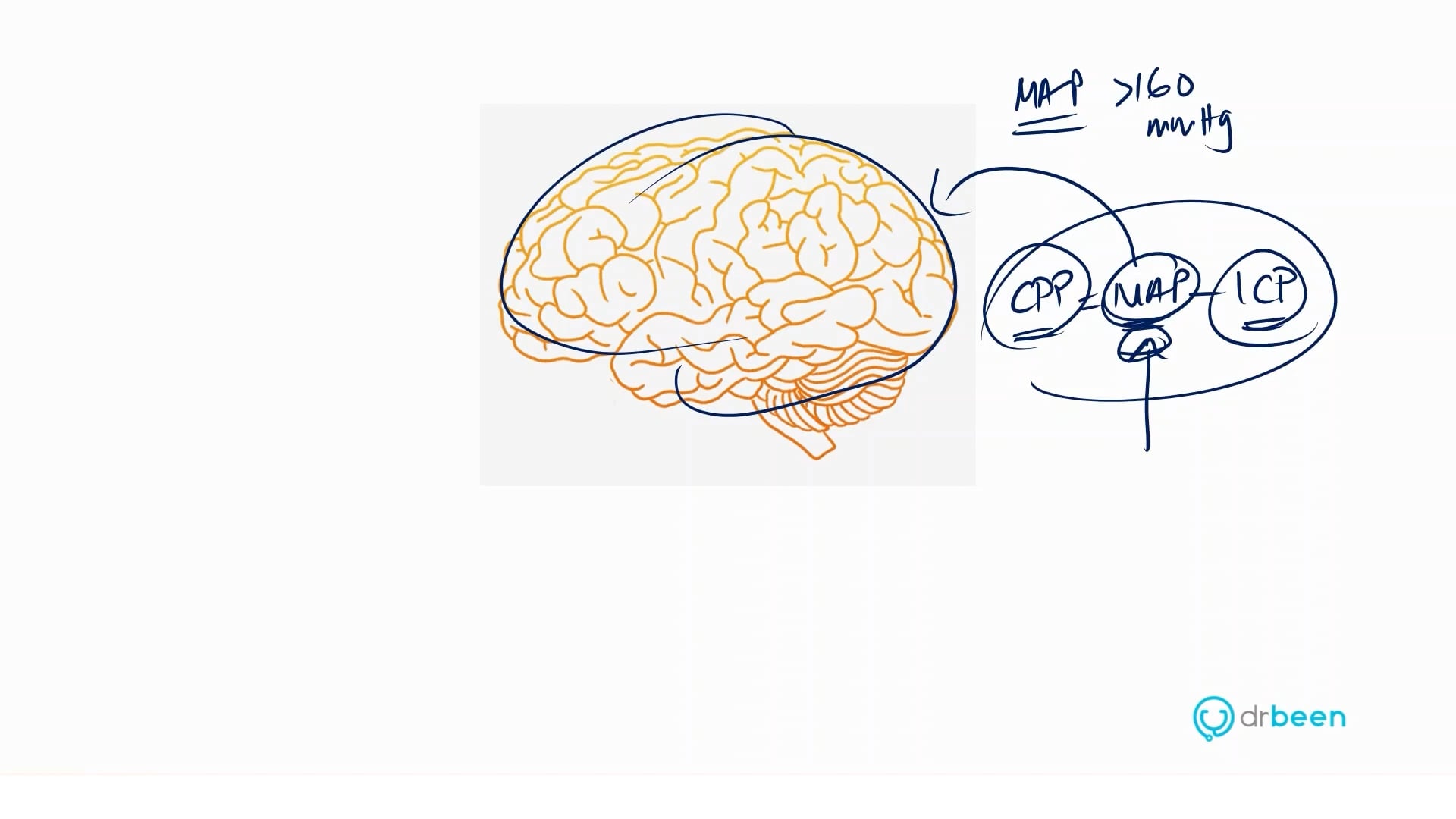
Questions from Katanje Phiri: The approach in management of stroke secondary to severe hypertension.....?
Questions from DrHaseeb Ubaid Ullah: Resistant recurrent hypertensive urgency treatment plan
And basic treatment plan of a patient with raised BP during early period of ischemic attack
Questions from Marlene Torres: There is an attributing factor of a patient having OSA will also lead to AFIB. But is OSA also an attributing factor of HTN?
Questions from Marlene Torres: There is an attributing factor of a patient having OSA will also lead to AFIB. But is OSA also an attributing factor of HTN?
Questions from Robert Adams: How does obstructive sleep apnea play a role in your treatment of a hypertensive patient? Do you screen and treat early or do you wait till later?
Questions from Robert Adams: I hope at this point we all know smoking is terrible for us, is vaping as bad? I’ve also read pot has 10x the nicotine as cigarettes, is nicotine the culprit and if so have we seen any changes in rates of atherosclerosis or hypertension in legalized vs non legalized states?
Questions from Robert Adams: Do you know of any new treatments, drug trials , implantable mechanical devices that are promising for hypertension?
In this video we will learn about:
Presented by Dr. Anam Tariq and Dr. Mobeen Syed
No credit card information needed.












Write A New Comment
1 Comments
kncburma@*.com
Apr 14 2020, 8:39 pm
what is management for patients who have normal BP after taking medicine but their BP is still high in morning before taking medicine?